Another analysis I wrote during the 2013 performance crisis in England’s A&E departments. Jeremy Hunt had just blamed the withdrawal of many GPs from providing out of hours (OOH) services for “rising attendance” and a whole range of other purported causes were being suggested. The debate since then has shifted but still lacks much grounding in actual facts. So what I said then is still worth reading.
I will update some of the analysis here in new posts when I can to show whether new evidence changes the picture (though it mostly doesn’t).
Apparently, our hospitals are being swamped by too many patients turning up in A&E. And the busy A&Es are now becoming slow and annoying places to go with the largest number of patients waiting more than 4hrs for a decade or so. It is about time something was done, is it not?
Indeed many people have weighed in to the debate with suggestions about exactly what needs to be done which range from Jeremy Hunt’s idea that the GP contract needs to be renegotiated (so they have to take back responsibility for out of hours services), through the idea we need to re-educate patients about what an emergency is, to the idea that we need a large increase in medical staffing to cope with the tsunami volume of attendances. And now there is a row about how much money needs to be spent to fix the mess.
Trouble is, nobody seems to have looked at the data to check what the problem is or when it started. Commentators are now behaving a little like doctors who prescribe treatments without either seeing the patient or checking their medical history.
While many commentators went straight to solutions, John Appleby and team at the Kings Fund bothered to look at the headline numbers (their numbers and a simple chart illustrating the mistake are here.
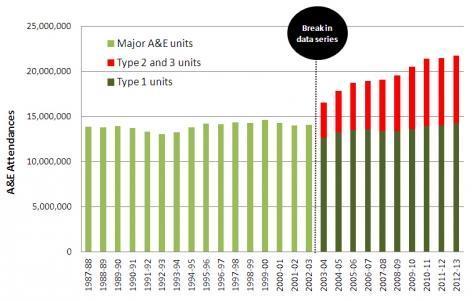
They pointed out that the apparent large increase in A&E volume since the GPs started opting out of OOH services was an artefact of another change that happened at the same time: we started opening new Minor Injury Units (MIUs) and Walk In Centres (WICs) and counting the numbers attending those. These don’t open 24 hrs a day so probably don’t deal with OOH refugees from GPs. They have attracted a large number of patients while the attendances in 24hr major A&Es has not changed much. This single piece of analysis undercuts any blame being passed to the GPs for the current problems in A&E.
Most other commentators have been misled by looking only at the total and assuming that major A&Es are being swamped. Interestingly, the Department of Health were advised not to focus on the aggregate data in the mid 2000s precisely because doing so obfuscates the location of performance problems; they chose to present the—better looking—aggregate only.
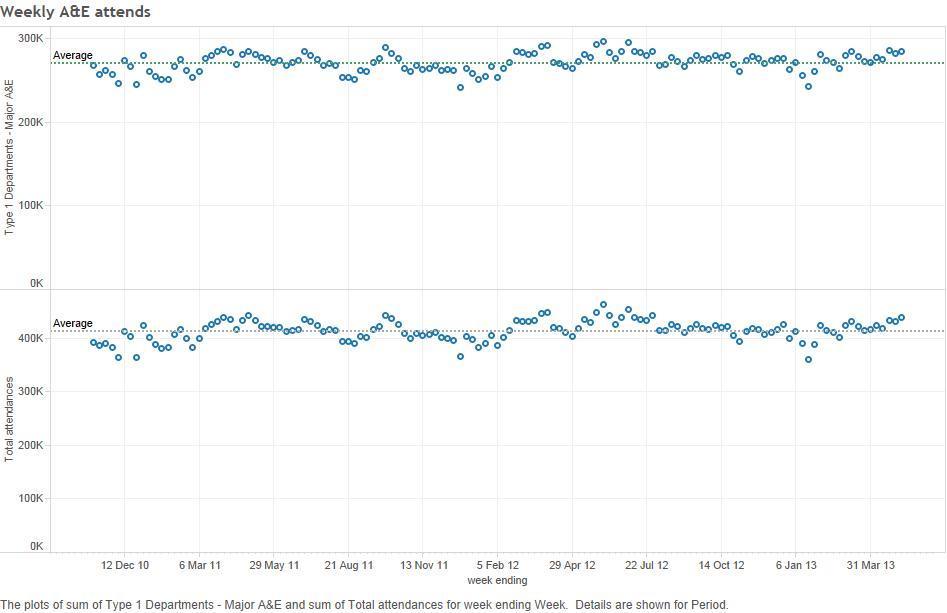
But there are further subtle versions of that theory being repeated. The HSJ reported on Thursday May 16 that an extra million people had attended A&E in 2012-13 compared to the previous year. But they forgot to put this in context. The rise was almost entirely the result of high attendance in the middle of 2012, so clearly unrelated to the current performance problems. Performance was much less of a problem in those weeks in 2012 with exceptional attendance. Here are the weekly numbers (total and major attendance):
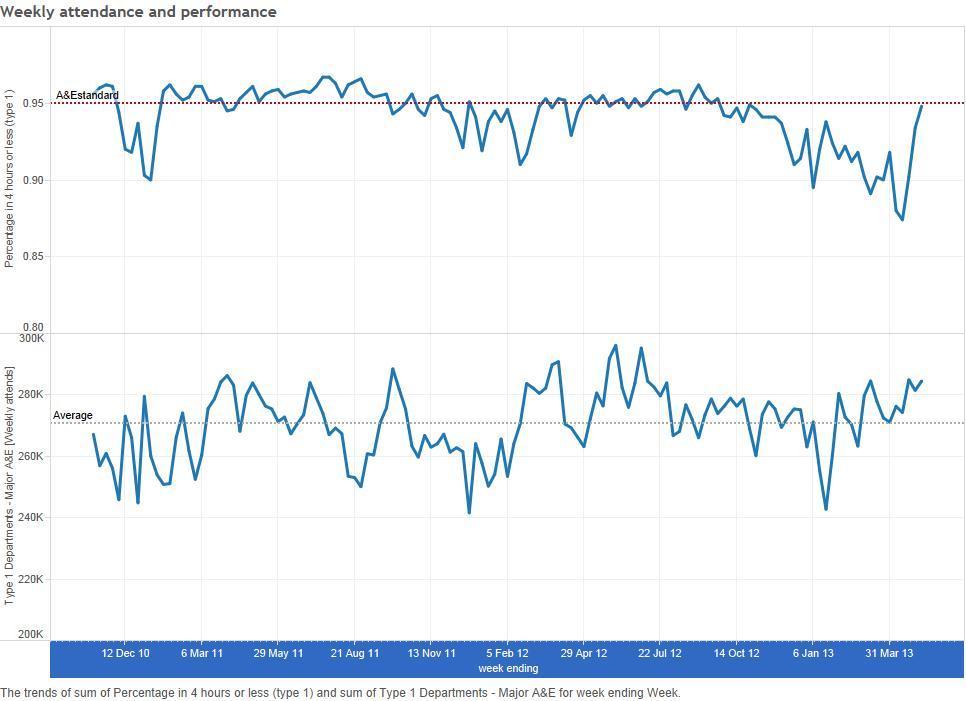
It is also worth looking at the more recent data in more detail. We looked at the weekly performance of and the weekly attendance at major A&Es. There is no apparent relationship between performance and the national volume in major A&Es where the performance problems exist:
People interested in the numbers might also want to look at the scatterplot of national performance versus attendance here as this makes the lack of relationship between the volume and performance even clearer:
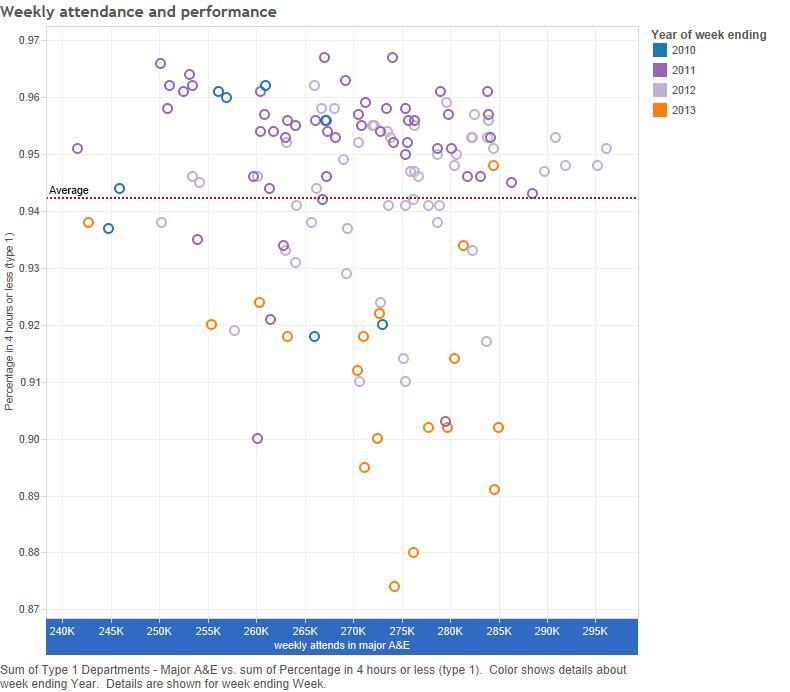
Note that weeks in 2013 are highlighted in orange clearly showing that poor performance is not associated with the volume.
We also looked at the same analysis for many individual trusts (an analysis we built in to the NHS Commissioning Board’s NHS England’s Integrated Intelligence tool). A few show vague relationships but most show nothing strongly suggesting that volume of attendance causes the performance problems.
Analysis taken from the more detailed HES dataset (which records when patients arrive, but is less recent) and some individual trusts also confirms that the problems don’t look related to out of hours care. Not least because A&Es are not that busy out of hours and that most problems occur during the day when GPs are open. Nor is there any indication that particular groups of patients, such as the infirm old are suddenly arriving in larger numbers.
What we can tell from this detailed analysis, though, is that the patients needing a bed are the biggest problem. We can also tell from the time of day and the day of the week that the problems occur that this has some relationship to how hospitals manage their beds.
So What?
So, overall, we have a performance problem but the plausible stories we have been discussing are not obviously compatible with the actual data. If they lead to actions or even policy changes then a) the changes won’t fix the problem and b) we have engaged in an act of story driven policy not evidence driven policy.
We have been here before. In 2005 the Healthcare Commission published a report analysing the factors related to A&E performance. Its main conclusion was that the obvious things that look like good explanations of poor performance (like too many attendances, too few staff…) don’t explain anything.
"…there is no relation at all between staffing levels and performance. Nor does any relation exist between changes in staffing and performance. None of the intuitively “obvious” factors that might be thought to influence performance seem to matter much.
… the way a department is organised has more influence on its performance than even major changes in staffing. In other words, management matters. And just increasing resources is a poor way to fix performance problems."
This incited much incredulity despite being an accurate summary of the regulator’s work.
We seem to have arrived at the same point again. We are identifying problems and proposing solutions neither of which are consistent with the evidence while ignoring known practices that work. Another report from Nigel Edwards agrees with this analysis.
I have no magic bullet to offer. But stepping back and looking at the data before proposing solutions based on nice theories that are inconsistent with the facts would probably help.
Here are some useful thoughts (based on years of A&E analysis and observation) that might help focus the debate:
- Just because the problem manifests in A&E doesn’t mean it is an A&E problem. If the problem is finding beds for emergency admissions, that is a hospital bed management problem not and A&E problem. Adding more doctors to A&E will make no difference at all to this.
- The plausible stories being told assume causality runs from volume to long waiting times. This feels right, but careful observation suggests it might be exactly the wrong way round. Long waits mean there are more people in the department so things feel busier despite the volume being perfectly normal. This is at least consistent with the statistics unlike the idea that too many attendances make things busy, which is not.
- Slow A&E processes don’t mean staff are not working hard enough. Poor processes are a problem of coordination across the staff and the different departments in the hospital. Poor coordination makes life worse for both staff and patients. This is, and I hate to use a dirty word but it is important, a management problem. A failure, for example, to coordinate hospital discharges (which the hospital can control) with the pattern of A&E arrivals (which they can’t control, much) will lead to long waits for many patients in A&E. A failure to segregate processes for patients needing simple treatments from those needing more medical time, will lead to long waiting times for all and much wasted medical effort that does nothing for the clinical quality or patient experience.
- While there are bed-blockers using up valuable beds because their social care is uncoordinated with their hospital care this is unlikely to be the primary cause of A&E blockage unless every hospital bed is blocked. In Most hospitals about 20% of the patients in beds will leave on any one day. The typical hospital will do a discharge round in the afternoon allowing consultants to sign those patients as fit to go home. Mostly those patients will be fit to leave in the morning but will occupy a bed for the day. Most hospitals where any analysis has been done could easily accommodate all their A&E admissions just by discharging patients first thing in the morning; most still don’t. Many have no clue as to who is in what bed or when they should leave (imagine if a hotel had to send porters to check whether any rooms were free when new guests arrive, that is the typical hospital).
- The NHS’s disdain for “bureaucrats” (which is an even dirtier word for “management”) leaves the system blind to many key causes of performance problems. Getting medical staff to work in a coordinated way across the whole hospital so the overall system works well is a management problem. Good management can make a huge difference to clinical quality, patient experience and the quality of the working day of all the medical staff. But improvement isn’t going to happen if we keep misidentifying the problem and assuming that management is a parasitic burden on the medical staff and not a lubricant to smooth their work and make it more effective.
No comments:
Post a Comment